Can't get by on a tampon?
You're not alone.
Yes, normal periods exist. Those who suffer from Abnormal Uterine Bleeding (AUB) don’t have them.
"C'mon! Just use a tampon!"
What is a “normal” period?
Periods vary from person to person. However, there is an average when it comes to the amount of blood loss during menstruation.1
*Bleeding before your first period (menarche), after menopause, or during pregnancy is not addressed in this overview of AUB
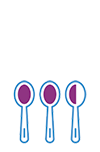
Typical menstruation
During typical menstruation, the uterus sheds 37-41mLs of blood over the first 5–7 days of the menstrual cycle
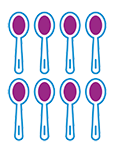
AUB menstruation
Women with AUB average 80mLs over a variable number of days
So, women with AUB bleed about 3 times more than women who don’t have AUB.
(If you use 16 or more regular tampons or pads with each period, that's not normal and there are treatments to help)

Up to one-third of women will experience AUB2
Chronic does not mean OK
Over time, many women accept or ignore symptoms of AUB. Some don’t have time to deal with it. Others can’t take off work to see a doctor or don’t believe there’s a treatment for them. While still others believe that it may be hereditary and there’s nothing that can be done.
These are all reasons why women delay getting a diagnosis.
But imagine how much easier life would be, and how much better you would feel, if you knew what was causing your symptoms. And you knew which treatment options were the best fit based on your exact diagnosis.
How do doctors diagnose AUB?
It depends on the doctor.
If you’re seeing a general practitioner, blood work may be the first and only step before they refer you to a gynecologist. Blood work can include ruling out pregnancy, checking your blood’s clotting capabilities, testing for anemia and measuring your thyroid levels.
When you see a gynecologist, you’ll be able to have a more thorough exam, which should be based on the PALM-COEIN classification system. It sounds complicated, but PALM-COEIN actually simplifies your AUB diagnosis. And it makes sure that everyone is speaking the same language.
PALM-COEIN System3
for Classification of Causes of AUB in the Reproductive Years.
P.A.L.M.
Polyps
Non-cancerous growths on the lining of the uterus and/or cervix
Adenomyosis
Endometrial tissue that is present within and grows into the muscular walls of your uterus
Leiomyoma (Fibroids)
Noncancerous growths of muscle in the uterus
Malignancy & Hyperplasia
Cancerous growths or atypical pre-cancerous endometrial tissue

C.O.E.I.N.
Coagulopathy
The blood’s ability to coagulate (form clots) is impaired
Ovulatory dysfunction
Abnormal, irregular (with ≤ 9 periods/year), or absent ovulation
Endometrial
Thickening of the lining of the uterus, or endometrium due to hormonal fluctuations
Iatrogenic
Caused by medical interventions (for example, the placement of an IUD) or certain medications
Not otherwise classified*
Rare conditions, or those not identifiable as related to the AUB symptoms
*Conditions to be included in not otherwise classified include pelvic inflammatory disease, chronic liver disease, and cervicitis.
Your AUB diagnostic consultation
The first step toward getting a diagnosis is to tell your doctor what your symptoms are, how they impact you during your menstrual cycle and any related family history.
The next step is to have an examination of your uterus.
How physicians see the uterine cavity
Hysteroscopy
To see the interior of the uterine cavity, physicians use a hysteroscope. With this tool, your physician directly views the inside of your uterus using a tiny camera attached to a thin wand. (Some gynecologists offer hysteroscopies in the office, which is really convenient.)
Ultrasound
Your gynecologist may choose to do a transabdominal ultrasound or a transvaginal ultrasound. This is a good start, but ultrasounds don’t show everything. And sometimes what they show can’t be classified.
Saline infusion sonography (Sonohysterogram)
During transvaginal ultrasound, your physician delivers saline into the uterine cavity through the vagina and cervix. This expands the cavity, enabling the physician to better see the ultrasound images of the uterus and any tissue growths, if present.
MRI
Not all causes of AUB are visible from within the uterine cavity, though. For example, some fibroids or endometrial tissue can be in the walls of the uterus. If your doctor doesn’t visually identify a cause in your uterus, they may suggest having an MRI, which will provide a much more detailed image of your whole uterus, not just the interior of the cavity.
All these efforts are designed to definitively diagnose the cause of your AUB. And that’s really important. Because when you are experiencing a health condition and don’t have a clear understanding of what’s happening in your body, you may experience stress. On top of AUB.
No one needs that.
How AUB impacts fertility4
The American Society for Reproductive Medicine notes there are several ways uterine fibroids and polyps can reduce fertility:
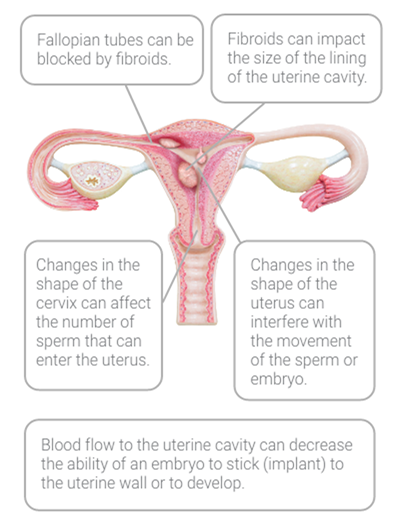
Though studies have not been conducted to confirm how polyps affect fertility, it is theorized that polyps interfere with or impede the planting of the embryo in the uterine lining.
How do you treat AUB?
In the past, the burden has been placed on women to manage a debilitating but treatable condition.
Left untreated, AUB often results in a hysterectomy.5
A hysterectomy is an invasive surgery with potential long term complications. Today, women have less invasive options, thanks to advancements in gynecologic care.
Now you can treat AUB without hormones, while preserving your uterus.
You deserve to be heard
A consultation with a gynecologist who understands AUB is what you need and deserve.
- 1.Abnormal uterine bleeding. The American College of Obstetrics and Gynecologists. Last accessed September 15, 2022. Abnormal Uterine Bleeding I ACOG
2.Davis E. Sparzak PB. Abnormal Uterine Bleeding [Updated 2022 Feb 10]. In StatPearis [Internet] Treasure Island (FL): StatPearis Publishing. 2022 Jan. Last accessed September 15, 2022. Abnormal Uterine Bleeding – StatPearis – NCBI Bookshelf (nih.gov)
3.Munro, M. G., Critchley, H . O., Broder, M. S., Fraser I. S., & FIGO Working Group on Menstrual Disorders (2022). FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. International journal of gynaecology and obstetrics the official organ of the International Federation of Gynaecology and Obstetrics. 113(1), 3-13. Last accessed September 15, 2022. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age – Munro – 2011 – International Journal of Gynecology & Obstetrics – Wiley Online Library
4.Fibroids and fertility. American Society for Reproductive Medicine. Fibroids and Fertility (reproductivefacts.org). Last accessed September 15, 2022.
5.Plotting the Downward Trend in Traditional Hysterectomy, https://labblog.uofmhealth.org. Last accessed September 15, 2022
Minerva Surgical does not provide medical diagnosis, treatment or engage in the practice of medicine. There are potential risks with any medical procedure. These procedures may not be appropriate for all patients, and all patients may not benefit. For information about risks, visit minervasurgical.com/safety . Rx Only.
Minerva The Uterine Health Company, Minerva ES, Symphion and Genesys HTA are registered trademarks of Minerva Surgical, Inc.
Resectr is a trademark of Minerva Surgical, Inc.
All other trademarks are property of their respective owners.
© Minerva Surgical, Inc. 4255 Burton Drive, Santa Clara, CA 95054. All rights reserved. K0123-02 Rev. B